Gallstones – Types, Causes, Symptoms, Prevention, Treatment
What are Gallstones?
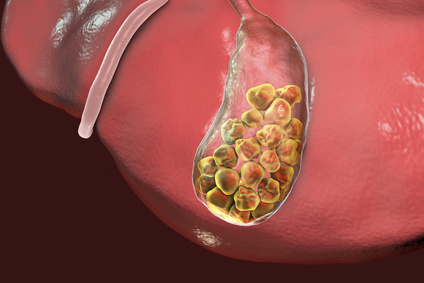
A gallstone is a small pebble that develops in the gallbladder often as a result of sediment from the bile. The medical term for a gallstone is a cholelith and the process of gallstone formation and the presence of gallstones in the gallbladder is known as cholelithiasis.
There are some less common types of gallstones that do not develop within the gallbladder but rather in the bile ducts (medical term : choledocholithiasis). Many gallstones exit the gallbladder and pass out with the bile. It often goes unnoticed. At times however, the gallstone may get stuck in the narrow neck of the gallbladder or within the bile duct itself.
Types of Gallstones
There are two types of gallstones – cholesterol or pigment. A third type known as a mixed stone is a combination of a cholesterol and pigment stone. Although the most common type of gallstone is a cholesterol stone, it does contain some characteristics of a pigment stone. A gallstone made purely of cholesterol is rare.
Cholesterol stones are a pale yellow in color but due to the components of a pigment stone, it appears darker yellow to a brownish-yellow. Pigment stones are generally brown or black – brown stones tend to form in the bile duct while black stones develop in the gallbladder
Cholesterol Gallstones
Cholesterol is a product of fat metabolism in the liver and is passed out with bile. Since it is insoluble, cholesterol binds with water-soluble bile salts and water-insoluble lecithin to exist as small micelles or vesicles (‘bubbles’) in the bile. Bile enters the gallbladder where it is stored and concentrated.

If the cholesterol concentration within the bile is too high, it may exceed the solubilizing capacity of the bile salts and precipitate. In addition, there is a diminished movement of bile, and mucus secretion within the gallbladder that allow the sediments to aggregate. For this reason, cholesterol stones almost always exist in the gallbladder.
Over time, the presence of bacteria and the action of the body’s immune cells breaks down bilirubin within the cholesterol stone and the chemical composition partially resembles a pigment stone. This is known as a mixed stone.
Features of Cholesterol Gallstones
Composition
- Apart from cholesterol, these gallstones also contain calcium salts – calcium phosphate, calcium bilirubinate, calcium carbonate. Mucin glycoprotein is also present and is the main compound that cements the stone.
Color
- Cholesterol gallstones appear yellow in color if they are made of pure cholesterol, which is rare, but due to the presence of calcium salts and hydrolization of conjugated bilirubin, it can appear dark yellow to brownish-yellow.
Quantity
- Cholesterol stones usually do not occur in isolation. Multiple stones may fill up the gallbladder and can be as large as several centimeters. Rarely, a single large cholesterol stone may be found.
Location
- Cholesterol stones are almost always found in the gallbladder.
X-Ray
- Most cholesterol stones are radiopaque and are detectable upon x-ray.
- A large stone made up of purely cholesterol, which is rare, can be radiolucent and therefore not detected upon x-ray.
Pigment Gallstones
Pigment stones occur when there are high amounts of bilirubin, particularly unconjugated bilirubin, in the bile. While bile does contain small amounts of unconjugated bilirubin, most of these bilirubin is conjugated. Unconjugated bilirubin occurs as a result of hemolytic anemias, where large amounts of red blood cells are broken down, or when bacteria within the biliary tree is able to hydrolyze the conjugated bilirubin due to the action of bacterial enzymes.
Black and Brown Pigment Stones
Composition, Color and Consistency
- Pigment stones can be classified as brown or black pigment stones. The changes in color may be due to the amount of calcium salts, like calcium bilirubinate, and cholesterol which also affects the consistency. Mucin glycoprotein is also present and is the main compound that cements the stone.
- Brown stones usually have a higher amount of cholesterol compared to black stones.
- Black stones typically have a higher concentration of bilirubin compared to brown stones.
- Brown gallstones are softer and and more greasy in consistency.
- Black stones are firmer but crumble easily.
Size and Quantity
- Pigments stones are usually smaller than cholesterol stones and are rarely larger than 1.5 centimters.
- Brown stones are more likely to occur in isolation while several black stones may be found in the gallbladder.
Location
- Black pigment stones are usually found in the gallbladder and is more likely to occur in cases of hemolytic anemias.
- Brown pigment stones are more frequently seen in the bile ducts and is commonly due to an infection.
X-Ray
- Most black pigment stones are radiopaque and can be detected upon x-ray.
- Brown pigment stones are often radiolucent and may not be detected upon x-ray.
Signs and Symptoms
Most cases of gallstones are asymptomatic meaning that there are no symptoms evident to the patient (silent gallstones). As the condition progresses, the signs and symptoms of gallstone disease may become evident, wither just the presence of pain (uncomplicated gallstone disease) or signs and symptoms due to complications like jaundice (complicated gallstone disease).
It is often thought that larger stones will cause more severe symptoms but it is the smaller stones and biliary sludge that are usually responsible for gallstone pain, attacks and the other signs and symptoms.
- Jaundice
- Obstructive jaundice is a result of obstruction of the common bile duct or in the cystic duct resulting in stricturing of the hepatic/common bile duct (Mirizzi’s syndrome)
- It results in yellowish discoloration of the skin, sclera (“whites” of the eye), mouth and deeper tissues.
- Pale or clay colored stools and dark urine may also be present.
- Pruritis – itching of the skin
- If the gallbladder is palpable and painless and the patient is jaundiced, then pancreatic or gallbladder cancer should be suspected (Courvoisier’s law).
- Fever
- The fever is usually low-grade or mild or occasionally high.
- Rigors with fever are not usually present, however, if it does occur along with a abdominal pain, ascending cholangitis should be suspected (Charcot’s triad).
- Nausea and vomiting
- Nausea accompanies the pain and is more frequent after eating food, not only fatty foods.
- It should not be confused with indigestion and other gastrointestinal causes of nausea and vomiting. No belching or bloating (sensation of fullness) is present in gallstones in contrast to gastrointestinal causes.
- Symptoms of acute pancreatitis
- Inflammation of the pancreas due to gallstones (gallstone pancreatitis) may occur as a result of the passing gallstone causing swelling of the ampulla of Vater.
- The stone may have already passed into the duodenum yet the symptoms of acute pancreatitis may persist.
- The signs and symptoms of acute pancreatitis may be very similar to a gallstone attack. Sweating, a rapid pulse and pain radiating to the back which is partly relieved by bending forward is typical of acute pancreatitis.
- Symptoms of intestinal obstruction
- Rarely, a large gallbladder stone may erode the gallbladder and enter the intestine where it causes intestinal obstruction.
- This is known as a gallstone ileus.
- It may result in prominent vomiting, constipation and ascites (swollen stomach) along with severe abdominal pain.
- A fistula or perforation of the gallbladder may also arise in complicated gallbladder disease resulting in the signs and symptom associated with these conditions.
Gallstone Pain
This is the most common symptom indicating the presence of gallstones (cholelcystoithiais ~ stone in the gallbladder, choledocholithiasis ~ stone in the duct). Gallstone pain is referred to as biliary pain or biliary colic which is a result of obstruction of the bile duct, or less frequently, of the gallbladder itself.

Gallstone pain becomes evident when the stone lodges in the duct, either the gallbladder duct (cystic duct) or the common bile duct. The gallstone(s) may pass out of the duct and the pain may resolve spontaneously. It is complicated by in inflammation of the duct(s) known as cholangitis.
Gallstone pain may also be a result of inflammation of the gallbladder (cholecystitis), which is another complication that may occur in conjunction with cholangitis or cholecystitis may occur on its own. Infection, particularly a bacterial infection, may cause or complicate a case of gallstones, cholangitis and cholecystitis.
Other complications associated with gallstones and gallbladder disease may also be a result of gallstone pain. This includes :
- Empyema – collection of pus in the gallbladder
- Hydrops, or mucocele – collection of fluid (water or mucus) causing distension of the gallbladder
Other complications are discussed below and include acute pancreatitis, intestinal obstruction, fistula or perforation.
Location
Most cases of gallstone pain is felt in the epigastrium (upper middle abdomen) and less frequently it my be experienced more laterally in the right upper quadrant (right hypochondrium, right lumbar/flank). Gallstone pain may refer to the tip of the right scapula, back, left upper quadrant (gastric pain) or chest. It is not uncommon for gallstone pain to be mistaken for peptic ulcers, gastritis or myocardial infarction (heart attack).
Gallstone Attack
Gallstone pain comes on suddenly and is very intense. It is described as excruciating and constant and may persist for anywhere between 30 minutes to 2 hours. In some cases, gallstone pain may persist for up to 5 hours. If it is persisting for 6 hours or more then cholecystitis or pancreatitis should be suspected.
Distension of the abdomen may also be noticed with gallstone pain. The gallbladder may be tender but it usually not palpable. A mass in the right upper quadrant (RUQ) mat be due to the omentum (part of the peritoneum) or bowel which becomes inflamed.
Murphy’s Signs
This is usually indicative of acute cholecystitis which is commonly due to gallstones. Two fingers (sometimes the entire hand) are used to apply pressure on the right upper quadrant. The patient is asked to breathe in. If this elicits pain leading to the patient to stop breathing in, then this is a positive Murphy’s sign. This can only be confirmed if the same technique does not elicit pain or discomfort in the left upper quadrant.
Causes of Gallstones
The formation and symptomatology of gallstones is well understood but the exact reason for many cases of gallstones, particularly cholesterol stones, is still unclear. There are known risks for the development of gallstones but despite the presence of these contributing factors, not every person will develop gallstones.
The classic clinical presentation is a patient who is fat, forty, female and fertile, which is also known as the 4 F’s for gallstone presentation. Another factor to consider is the fifth F which stands for fair in reference to Caucasians, particularly those of north European descent (“fair skin, fair hair”). However, this does not encompass all the risk factors associated with the development of gallstones.
Cholesterol stones, which are the most common type of gallstones, form when the cholesterol levels in the bile exceeds its solubilizing capacity. This means the the bile is no longer able to hold cholesterol in suspension and it precipitates. With time the sediments aggregate to form stones.
Pigment stones are more frequently linked to infections and biliary stasis (impaired outflow of bile). It is associated with large amounts of unconjugated bilirubin in the blood.
Advancing age is one of the main risk factors in both types of gallstones. Previously it was believed that obese middle-aged Caucasian women (fat, female, forties, fertile, fair) were the highest risk group but with time a number of other risk factors were attributed to the likelihood of developing gallstones.
Causes of Cholesterol Stones
Cholesterol stones form when the amount of cholesterol in the bile exceeds its solubilizing capacity. Cholesterol is a normal product of fat metabolism in the liver and is excreted in the bile. Since it is insoluble in water, it is held in suspension by the water-soluble bile salts and water-insoluble lecithin as micelles or vesicles. When the quantity of bile salts is insufficient to hold cholesterol in suspension, cholesterol sediments start aggregating together with the help of mucus from the gallbladder to form cholesterol stones.
Risk Factors for Cholesterol Stones
- Age – older age groups.
- Ethnicity – northern Europeans, north and south Americans, including Caucasians, Hispanics and Native Americans.
- High triglyceride and low HDL levels in the blood – hyperlipidemia.
- Female. Apart from gender, the use of female hormone medication like oral contraceptives, and pregnancy increases the risk of gallstone formation.
- Metabolic syndrome
- Obesity
- Rapid weight loss
- Fasting or dieting and other factors that slows gallbladder emptying like neurological defects as a result of injuries to the spinal cord.
- Other factors such as a family history, diet high in fats and sugars, drugs like cholesterol-lowering agents and certain chronic conditions like diabetes may also increase the risk for cholesterol stones.
- Inborn errors in bile acid metabolism, like cerebrotendinous xanthomatosis
Causes of Pigment Stones
Pigment stones are a result of large amounts of unconjugated bilirubin in the blood. Most bilirubin in the bile is conjugated with only a small amount being unconjugated. Any factor that increases the amount of unconjugated bilirubin may result in pigment gallstones. Bacterial enzymes, rapid and excessive breakdown of red blood cells and impaired bile flow or static bile are the main contributing factors.
Risk Factors of Pigment Stones
- Advancing age and ethnicity is also a risk factor – pigment stones are more commonly seen in Asians, particularly those living in a rural setting.
- Chronic hemolytic syndromes – this is the breakdown of red blood cells that is above the norm (black stones)
- Hepatic cirrhosis (black stones)
- Gastrointestinal diseases or surgery that impairs the resorption of bile salts (black stones)
- Impaired emptying of the gallbladder or static bile (brown stones)
- Infection, particularly bacterial or parasitic infections of the biliary tree (brown stones)
Prevention of Gallstones
Understanding and identifying the risk factors for gallstone formation is one of the key components of prevention. However, it does not mean that every person with these risk factors will develop gallstones. Generally, a single episode of symptomatic gallstones warrants the surgical removal of the gallbladder (cholecystectomy) in order to prevent a recurrence. This surgery however may be delayed until there is one or more recurrence and depends on the type of gallstone.
The link between diet and gallstone formation is inconclusive but avoiding fatty foods, dairy and meat may be useful in preventing gallstones. With high triglyceride levels being one of the risk factors of developing the more common type of gallstone, cholesterol stones, a triglyceride diet and proper management of hyperlipidemia should be considered. Obesity should also be targeted with proper medical weight loss.
Read more on the Gallstones Diet for dietary management and prevention of gallstones and foods to avoid.
Treatment of Gallstones
Proper diagnosis of gallstones with blood tests, imaging techniques like an x-ray, CT scan or HIDA, as well as endoscopic investigation is necessary before medical or surgical intervention is considered.
Read more on Gallbladder Tests.
Treatment of gallstones may involve one or more of the following measures :
- Medication
- Bile acid drugs like chenodiol or ursodiol helps to “dissolve” cholesterol stones.
- Lithotripsy
- Fragmentation of stones (“blasting”) using sound shock waves is known as lithotripsy. However a cholescystectomy may still be advisable and lithotripsy may therefore be unnecessary.
- Surgery
- Cholecystectomy (surgical removal of the gallbladder) is advisable for gallbladder stones.
- An ERCP with sphincterotomy or choledocholithotomy will be considered for bile duct stones.
Read more on Gallstones Treatment for information on different therapeutic options.
References
- Gallstones. Medscape
- Gallstones. University of California San Francisco




