What Is Staphylococcus aureus?
Staphylococcus aureus
Staphylococcus aureus (Gk. staphyle = bunch of grapes; Lat. coccus = spherical bacterium, aureus = golden) or golden staph (pronounced ‘staff’) is the most common species of staphylococcus bacteria causing infections in human.
Lab Tests for Staph
Staph Epidemiology
Staph Infections
S.aureus lives as a part of the normal skin flora in the nose or on the skin in 20-30% of healthy people (staph carriers), (1). However, in even slightly injured skin or mucosa, staph may cause styes, pimples, folliculitis, furuncles, boils (Picture 1), swimmer’s ear, sinusitis, epiglotitis, whitlow, breast infection, impetigo, cellulitis, genital infection, scalded skin syndrome or other staph infections. Infections of internal organs include urinary tract infections, arthritis, pneumonia, infection of veins (thrombophlebitis), lymph nodes (lymphadenitis) or lymph vessels (lymphangitis), bone infection (osteomyelitis) (Picture 2), or life threatening sepsis (staph blood invasion), infection of heart valves (endocarditis), meningitis, “flesh eating bacteria” infection (necrotizing fasciitis) and toxic shock syndrome. S.aureus enterotoxins may cause food poisoning.
S.aureus and S.epidermidis are among the most common causes of hospital-acquired infections, like bloodstream infections, infections of surgical wounds or pneumonia (2). Staph may also appear in vascular and urinary catheters, prosthetic joints and heart valves.
Staph skin infection usually appears as a red, warm, painful swelling with a blister, ulcer, or crust, and a drainage (Picture 1). Infection may spread into the deeper tissues, like the bones (Picture 2).
 |  |
| Picture 1. A boil on the upper arm | Picture 2. X-ray of child’s legs: osteomyelitis in shin bones (grey patches) |
How Widespread and How Dangerous is Staph?
Staph does not just float around in the air. A close skin contact, sharing towels, sport equipment and other fomites with an infected person or staph carrier, is needed to catch the infection. In an otherwise healthy persons staph usually causes only localized skin infections, which heal on their own within a few weeks (3). In heavily ill or immunodeficient patients, staph may cause deadly sepsis.
Staph Antibiotic Resistance
In 1942, only two years after introducing penicillin into infection treatment, staph resistance to penicillin was recognized in hospitals (4). In 1960, methicillin (later replaced by oxacillin) was used to treat penicillin resistant staph. Over 90% of staphylococci now contain enzyme penicillaze (which breaks down penicillin), so they have to be treated with penicillase-resistant penicillins, cephalosporins or other antibiotics (5).
MRSA
Methicillin Resistant S.aureus (MRSA) is resistant to most antibiotics derived from penicillin, including methicillin, so it has got a nickname ‘superbug’. MRSA was first detected in Britain in 1961 and is now increasingly recognized in the community worldwide (4). MRSA still mainly occurs in hospitals and nursing homes, but has lately spread to general community (Community Associated MRSA or CA-MRSA). It is impossible to distinguish MRSA from the “common” S.aureus (MSSA = Methicillin Susceptible S.aureus) only from symptoms (6). MRSA itself is not more “powerful” than MSSA, but it can be dangerous when it is not recognised as MRSA and not treated with appropriate antibiotics.
VISA and VRSA
In 1996, in Japan, S.aureus that was resistant to to an usual dose of vancomycin, was recognized. The terms Vancomycin Intermediate S.aureus (VISA) and Vancomycin Resistant S.aureus (VRSA) are now used, when 8-16 µg/ml or > 32 µg/ml of vancomycin respectively, is needed to inhibit staph growth during antibiotic susceptibility test (7). VISA and VRSA are not more powerful than other staphylococci, but they should be recognised as such, otherwise the treatment may not be successful. At present, VISA may be treated with larger doses of vancomycin and VRSA by some other antibiotics. VRSA is still rare: only seven cases were identified in United States between y. 2002-2006 (8).
Taxonomy of Staphylococcus aureus
Taxonomy (Gk. taxis = arrangement; -nomia= method) is classification of organisms in groups, according to their presumed natural relationships. In the “Bergey’s Manual of Systematic Bacteriology” Staphylococcus aureus is placed into:
Kingdom Bacteriae,
Phylum (Division) XIII. ‘Firmicutes‘ (Lat.: firmus = strong, cutis= skin, referring to the cell wall),
Class I. ‘Bacilli‘,
Order I. ‘Bacillales‘,
Family.VIII ‘Staphylococcaceae‘,
Genus I. ‘Staphylococcus‘
Species ‘Staphylococcus aureus’ (9).
Staphylococcus aureus Characteristics
S.aureus is a spherical (coccus) Gram-positive bacterium, about 1 micrometer in size, with the thick cell wall and thin capsule. It does not form spores, but it can still survive outside the body, for example, on bed lining or computer keyboards from few days to several weeks (10). It is a facultative anaerobe – it grows in the air, but can also thrive in anaerobic conditions. It is an opportunistic pathogen – it may be present in the body without causing any harm, but in lowered immunity or injury, it may cause a disease. Staph bacteria have no flagella, so they are immobile. They grow in pairs, short chains or clusters (Picture 3).
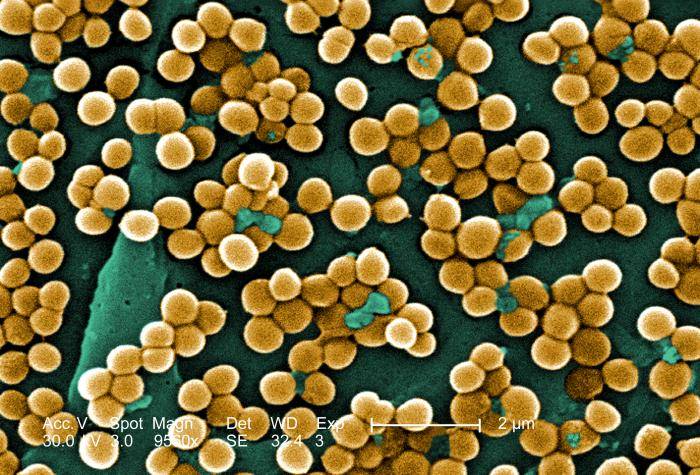
Picture 3. Grape-like clusters of S.aureus, electron micrograph, Magnitude. ~ 5000x;
(source: phil.cdc.gov)
S.aureus has ability to clot plasma – it is coagulase positive. Bacteria are resistant to temperatures as high as 122 °F (50°C), to high salt concentrations (<10%), and to drying (11). Colonies are usually 6-8 mm in diameter, rounded and smooth, golden yellow or pale yellow to orange (Picture 6).
Staphylococcus aureus Cell Wall Structure
A S.aureus wall consists from three layers: an outer polysaccharide capsule, peptidoglycan (murein) layer, and inner cytoplasmic membrane. Into this structure, proteins and teichoic acid are embedded and protrude from the cell wall on its outer side, forming a “fuzzy coat” (Picture 4), (12). Capsule is thin and may be seen only under the electron microscope. Sometimes more bacteria share one capsule and form a slime layer or biofilm, mostly found on the inner wall of venous and urinary catheters (13).
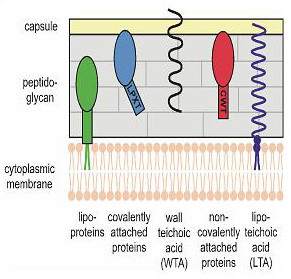
Picture 4. S.aureus cell wall structure
Virulence Factors of Staphylococcus aureus
A term ‘virulence’ refers to microbe’s “ability to invade the tissues of the host”, or “the potential to cause a disease”. Virulence factors of S.aureus include:
- Surface proteins that promote attachment of staphylococci to the damaged host tissues;
- Inhibitors of phagocytosis: capsule; Protein A that binds IgG molecules the wrong way and thus disrupt phagocytosis (14); polysaccharides secreted by staph aureus may form a biofilm or slime layer on indwelling medical devices (13); yellow pigment made of carotenoids protect bacteria against free radicals, and catalase breaks down peroxide (phagocytes use free radicals and peroxide to kill bacteria) (15);
- Bound coagulase – “clumping factor”, which causes coagulation of plasma and bacteria clumping, and free coagulase, which also triggers plasma coagulation (14);
- Invasins, which promote bacterial spread in tissues: kinases, hyaluronidases (destroy hyaluronic acid in the connective tissue), and fatty acid modifying enzyme (FAME);
- Cytotoxinsthat lyse cell membranes: hemolysins (lysis of erythrocites), leukotoxin and Panton-Valentine leukocidin – PVL (lysis of leukocytes);
- Exfoliatin Toxin – ET(in scalded skin syndrome), and superantigen toxins, which may trigger massive non-specific T-cell response: enterotoxins SEA-G (in food poisoning), and TSST-1 (in Toxic Shock Syndrome) (14);
- Antibiotic resistance – inherited and acquired. More details about S. aureus virulence factors.
NOTE: amount of virulence factors may differ among individual S.aureus bacteria considerably.
Prevention of Staphylococcus aureus Infections
Staph infection may be prevented on many levels:
- Hands washing and regular bathing.
- Skin wounds should be cleaned and covered.
- Food workers should be tested for staphylococci and being treated, even if they have no active infection. Staph carriers should not work in food preparation.
- Surfaces in hospitals can be cleaned with alcohol, quaternary ammonium or iodine compounds, which are effective to both MSSA and MRSA (20). Effective sprays for air disinfection also exist (16).
- Cows should be regularly checked for mastitis, and milk tested for S.aureus or its toxins. Only pasteurized or cooked milk should be used.
- Human and bovine vaccines against S.aureus have been developing.
What is NOT NEEDED to prevent staph infections: antibacterial soaps, wearing masks, washing linens of staph infected persons separately from others, using disposal dishes, disinfecting surfaces with hypochlorite, denying patients from using whirlpools or foot baths, work restrict staff members who are MRSA carriers, unless they have skin lesions or active nasal infection (20).
Treatment of Staphylococcus Aureus Infections
Staph colonization may be treated with mupirocin (Bactroban) nasal gel, and daily Hibiclens skin cleanser baths (17).
Local skin infections are treated with antibacterial ointments. In more extensive infections, S.aureus has to be tested for antibiotic sensitivity, and then usually oral antibiotics are used. Skin abscesses often have to be drained, and deep abscesses may require surgical drainage. In systemic infection, hospitalization and intravenous antibiotics are needed. Artificial heart valves and vein catheters often need to be removed or replaced.
Severe staph infections require treatment with parenteral penicillinase-resistant penicillin like nafcillin and oxacillin, or cephalosporins of 1st or 2nd generation (e.g. cephalexin, cefuroxime) plus clindamycin. Vancomycin is reserved for MRSA and clindamycin resistant strains or for life-threatening infections. Staph food poisoning usually heals on its own. List of antibiotics that can be used in Staphaureus infections (5, 11):
- Amoxycillin;
- Cefazolin, Cephalexin, Cephalotin;
- Ciprofloxacin;
- Clindamycin;
- Cloxacillin;
- Daptomycin;
- Dicloxacillin;
- Erythromycin (only for minor skin infections, since it is only bacteriostatic)
- Flucloxacillin (side effect: hepatic cholestasis);
- Linezolid (C);
- Methycillin (common adv. effects: hypersensitivity, interstitial nephritis);
- Minocycline (D);
- Mupirocin;
- Nafcillin;
- Oxacillin;
- Quinupristin/dalfopristin (Synercid) (C);
- Penicillin G (Benzylpenicillin), Penicilin V (Phenoxymethylpenicillin);
- Retapamulin;
- Rifampin (C);
- Tigecycline (D);
- Trimethoprim-sulfamethoxazole (C);
- Vancomycin.
NOTE: safety of group C antibiotics in pregnancy is not confirmed; group D antibiotics are unsafe in pregnancy.
Detailed intravenous and oral antibiotic treatment regimes in staph infections
Literature about Staphylococcus aureus:
Books:
- Staphylococcus: Molecular Genetics
Publisher: Caister Academic Press
Edited by: Jodi Lindsay Department of Cellular and Molecular Medicine, St George’s, University of London, UK
Publication date: May 2008
ISBN: 978-1-904455-29-5 - Staphylococcus aureus Infections
Author: Lisa Freeman-Cook and Kevin D. Freeman-Cook
Publisher: Facts on File (September 01, 2005)
ISBN: 9780791085080 - Methicillin-Resistant Staphylococcus Aureus (MRSA) Protocols
Author: Yinduo Ji
Publisher: Humana Pr Inc (December 30, 2007)
ISBN: 9781588296559 - Bergey’s Manual of Determinative Bacteriology, 9th ed.,
Author: Williams & Wilkins.
ISBN 0-683-00603-7
Related Articles:
References:
- Staph infections (Merck.com)
- Hospital acquired infections (Emedicine.com)
- Antibiotics for stapgh infection (Antimicrobe.org)
- MSSA and MRSA cannot be distinguished clinically (Garetthealth.org)
- VRSA (Utah.gov)
- VRSA incidence (Ncbi.nlm.nih.gov/pubmed)
- Taxonomy of S.aureus, Bergey’s manual (Bergeys.org)
- MRSA survival time on surfaces (Livescience.com)
- Staph salt and temperature resistance (Emedicine.com)
- S. Aureus – cell wall structure (Pubmedcentral.nih.gov)
- Staph biofilm (CDC.gov)
- Sprays for air disinfection (BBC.co.uk)



